Impetigo is the most common bacterial infection in children, which is highly contagious. It presents as an acute infection of the superficial layers of the epidermis and is caused by Group A Beta Streptococcus pyogenes(GABHS) or Staphylococcus aureus. Methicillin-resistant S aureus (MRSA) has also been reported to cause impetigo. S aureus accounts for approximately 80% of cases, GABHS accounts for 10% of cases. Systemic symptoms are usually absent. Regional lymphadenitis may occur.
Intact skin is usually resistant to colonization or infection by S aureus or GABHS.
Factors that can modify the usual skin flora and facilitate transient colonization by GABHS and S aureus include high temperature or humidity, young age, recent antibiotic treatment or any pre-existing cutaneous disease such as –
- Frequent Scratching
- Varicella/ Herpes simplex/Scabies/Pediculosis
- Thermal burns/Surgery/Trauma
- Insect bites
- Immunosuppression (systemic corticosteroids, oral retinoids, chemotherapy, HIV infection).
GABHS can be detected in the nose and throat of some individuals 2-3 weeks after impetigo lesions develop, although they do not have symptoms of streptococcal pharyngitis because impetigo and pharyngitis are caused by different strains of the bacteria. Acute poststreptococcal glomerulonephritis is a rare complication of nonbullous impetigo from nephritogenic strains of GABHS
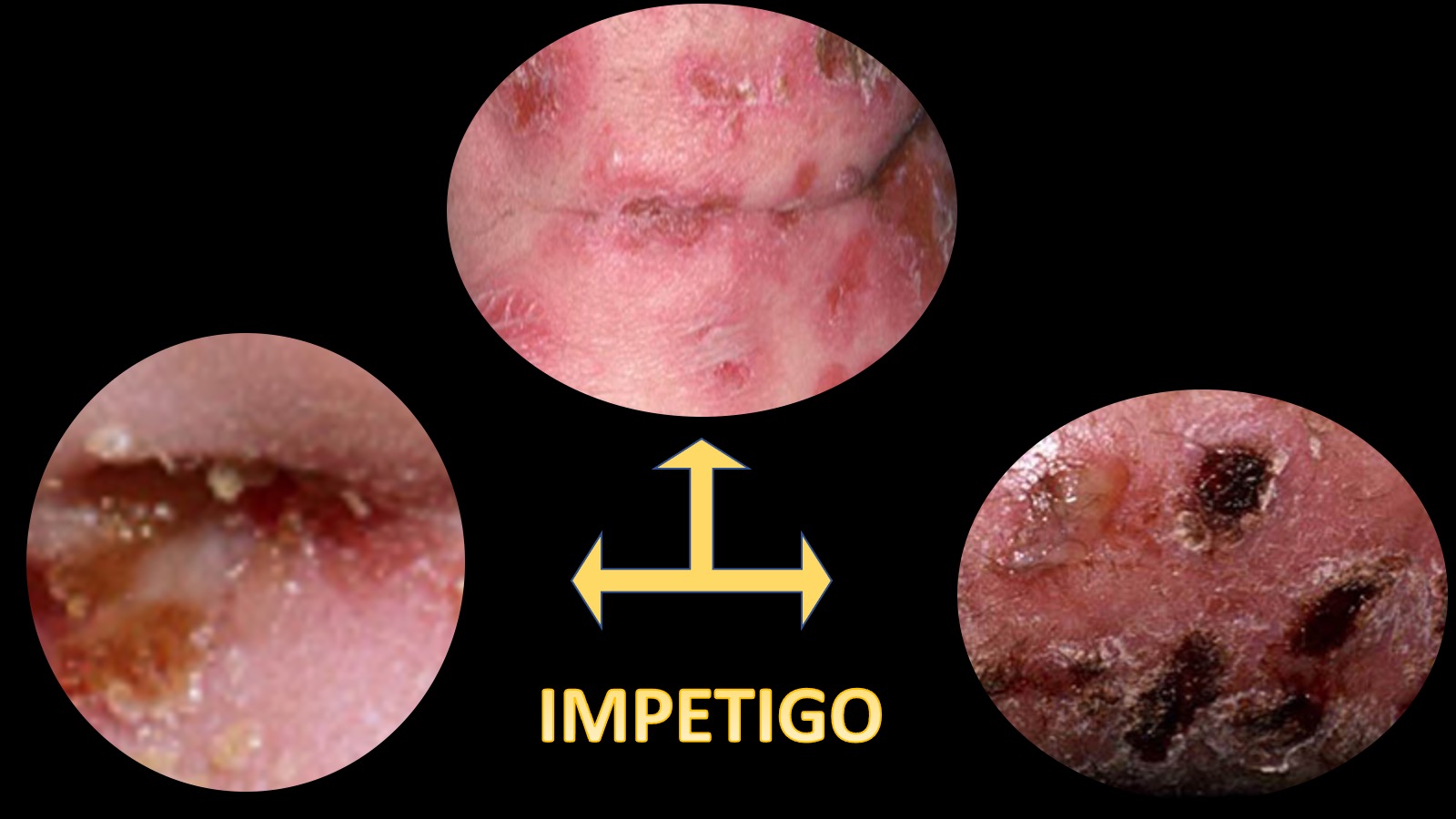
Variants of impetigo include
- Non-bullous impetigo (impetigo contagiosa) – the most common form
- Bullous impetigo
- Ecthyma
Next post: Non bullous impetigo
